Abstract
Since Danzer described it in 1919, the cardiothoracic ratio (CTR) has been the most widely used quantitative index of heart size on chest radiography: inexpensive, reproducible, and easy to automate, yet fundamentally an indirect surrogate derived from a two-dimensional projection. A recent study (Shen et al., JMRI 2026) extends the CTR to a new setting — measuring it on the abdominal MRI that ADPKD patients routinely undergo for total kidney volume (TKV), in order to identify left ventricular hypertrophy (LVH): opportunistic cardiac screening on an already-acquired scan. This article reviews the measurement definition and diagnostic performance of the CTR, focuses on its value for cardiac screening in ADPKD, and looks ahead to automated, three-dimensional quantitative measurement.
1. What the CTR measures
The CTR is defined as the ratio of the maximum transverse cardiac diameter to the maximum internal thoracic diameter:
CTR = (maximum right + maximum left cardiac diameter from the midline) ÷ maximum internal thoracic diameter
On a standard posteroanterior (PA), erect, full-inspiration chest radiograph in adults, a normal CTR is below 0.5; above 0.5 defines an enlarged cardiac silhouette. Its longevity has clear reasons: an intuitive threshold, almost no added cost, good reproducibility, and a clean geometric definition that lends itself naturally to automated segmentation and computation.
2. Diagnostic performance: a sensitive but non-specific screen
As a surrogate for cardiac enlargement confirmed by echocardiography or cardiac MRI, the CTR behaves like a typical screening index: broadly accessible but limited in specificity. An enlarged cardiac silhouette can arise from causes other than chamber dilation (pericardial effusion, epicardial fat, mediastinal mass, patient rotation), and in concentric hypertrophy — thickened myocardium without a dilated chamber — the CTR can be entirely normal. Its appropriate role is therefore screening and longitudinal follow-up, not definitive diagnosis or functional assessment.
Its main systematic error comes from technique: an anteroposterior (AP) projection magnifies the heart, and supine positioning or shallow inspiration bias it the same way — which is why the CTR on portable AP films is the most prone to over-reporting. Understanding these biases is a prerequisite for reading the number correctly.
3. Why the heart matters in ADPKD
Autosomal dominant polycystic kidney disease (ADPKD) is not only a kidney disease. Early-onset hypertension is one of its most common early features and drives left ventricular hypertrophy (LVH); LVH is an important predictor of cardiovascular morbidity and mortality in ADPKD. Early identification of cardiac involvement in this population therefore has clear clinical value.
The obstacle is cost and workflow: the reference standards for LVH are echocardiography or cardiac MRI, which require an additional test and appointment. Yet ADPKD patients already undergo abdominal MRI regularly to monitor kidney-volume growth (TKV) — a natural opportunity to assess the heart from imaging that has already been acquired.
4. Key advance: measuring the CTR on abdominal MRI to identify LVH
Shen et al. (JMRI 2026) seize precisely this opportunity: measuring the CTR directly on the abdominal MRI acquired for TKV in ADPKD patients, and using it to identify LVH. Its significance lies in:
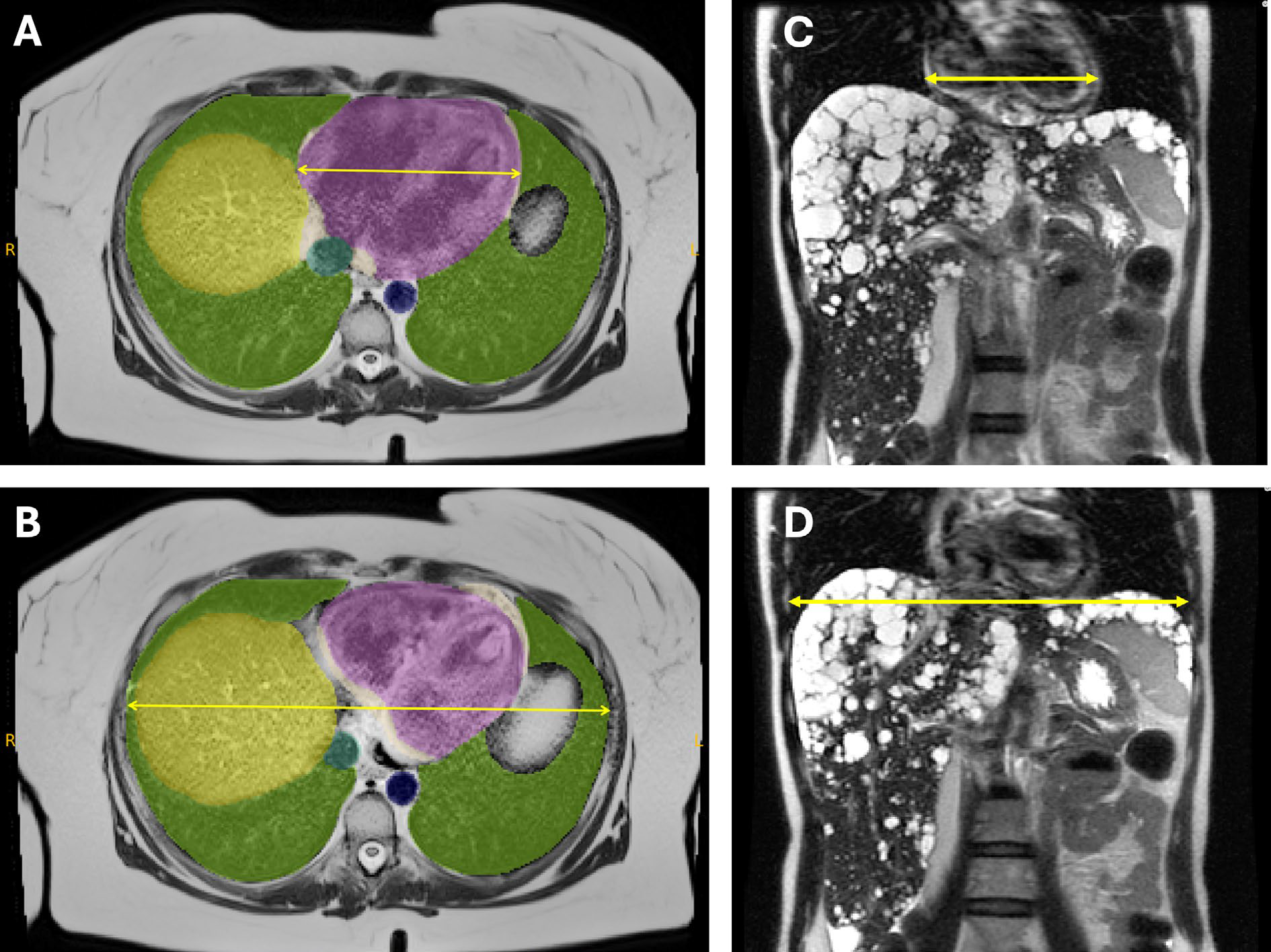
Figure 1. Measuring the cardiothoracic ratio on abdominal MRI in ADPKD. A, B (axial): the maximum transverse cardiac diameter and the maximum internal thoracic diameter; C, D (coronal): the corresponding measurements. Colour overlays are organ segmentations (heart, lungs, liver, etc.). Adapted from Shen et al., JMRI 2026.
Opportunistic screening — extracting an additional cardiac biomarker from an existing scan, with no added test, appointment, or radiation (MRI uses none).
Workflow fit — the measurement sits on the longitudinal follow-up pathway ADPKD patients already follow, and can be tracked alongside TKV.
A low-barrier index — the CTR is simple to define and to automate, suiting large-scale use across follow-up cohorts.
This also corrects a common impression — the CTR does not belong to chest radiography alone. As an inexpensive, reproducible morphological surrogate, it can be “carried over” to cross-sectional imaging acquired for other purposes, in the service of opportunistic screening.
Note: the cited work is a Research Letter; this article describes only its research premise. Refer to the original publication for specific diagnostic thresholds and performance metrics.
5. From a two-dimensional ratio to quantitative, automated measurement
The CTR exists to compensate for the limits of a two-dimensional projection. Cross-sectional and three-dimensional imaging can provide more direct cardiac quantification (chamber volumes, left ventricular mass, great-vessel diameters, epicardial fat), which does not depend on projection geometry and is more precise. But the distinctive value of the CTR is its very low cost of measurement and interpretation — when the goal is low-cost first-pass screening across large volumes of existing images, an automatable morphological ratio is exactly the pragmatic compromise that both engineering and clinical practice can adopt.
For precise characterization and functional assessment, favour three-dimensional quantification (volumes, mass, coronary calcium, etc.).
For opportunistic first-pass screening and follow-up on existing images, an automated CTR offers a cost-effective entry point.
Automating and standardizing the CTR, and embedding it in the longitudinal imaging follow-up of ADPKD, aligns with the direction TraceOrg represents: moving from eyeballing images to reproducible, quantitative measurement.
6. Conclusions
The CTR is a century-old, low-cost morphological surrogate for heart size: normal below 0.5 on an adult PA erect film; its weaknesses are non-specificity and dependence on projection technique.
ADPKD is prone to LVH through early-onset hypertension, and patients already undergo abdominal MRI regularly — creating the conditions for opportunistic cardiac screening.
Shen et al. (JMRI 2026) show that the CTR can be measured on abdominal MRI to identify LVH, bringing this classic index into the ADPKD follow-up setting.
The broader direction is automation plus quantification: embedding reproducible indices like the CTR into existing imaging workflows, while retaining three-dimensional quantification for precise assessment.
This article is a research overview and does not constitute medical advice. For specific diagnosis and treatment, follow the guidance of a qualified physician.
References
Shen M, Xiong Q, Wang Y, Blumenfeld JD, Zhu C, Hu Z, Bazojoo V, Sharbatdaran A, Csernus E, Prince MR. Cardio-Thoracic Ratio for Detecting Left Ventricular Hypertrophy on Abdominal MRI in ADPKD. Journal of Magnetic Resonance Imaging. 2026 (online ahead of print). doi:10.1002/jmri.70364.
Danzer CS. The cardiothoracic ratio: an index of cardiac enlargement. American Journal of the Medical Sciences. 1919. — the original description of the CTR (historical reference).